Carbetocin 100 mcg/mL.
Excipients/Inactive Ingredients: L-methionine, Succinic acid, Mannitol, Sodium hydroxide for pH adjustment, Water for injections.
Pharmacotherapeutic group: Oxytocin and analogues. ATC code: H01BB03.
Pharmacology: Pharmacodynamics: The pharmacological and clinical properties of carbetocin are those of a long acting oxytocin agonist.
Like oxytocin, carbetocin selectively binds to oxytocin receptors in the smooth muscle of the uterus, stimulates rhythmic contractions of the uterus, increases the frequency of existing contractions, and raises the tone of the uterus musculature.
On the postpartum uterus, carbetocin is capable of increasing the rate and force of spontaneous uterine contractions. The onset of uterine contraction following carbetocin is rapid after intravenous or intramuscular administration, with a firm contraction being obtained within 2 minutes.
A single 100 micrograms intravenous or intramuscular dose of carbetocin administered after the delivery of the infant is sufficient to maintain adequate uterine contraction that prevents uterine atony and excessive bleeding comparable with an oxytocin infusion lasting for several hours.
Clinical efficacy and safety: The efficacy of carbetocin in the prevention of postpartum haemorrhage due to uterine atony following Caesarean section was established in a randomised, active controlled, double-blind, double dummy, parallel-group trial designed to establish the efficacy and safety of carbetocin compared to oxytocin 25 IU. Six-hundred fifty-nine healthy pregnant women undergoing elective Caesarean section under epidural anaesthesia received either carbetocin 100 μg/ml as an IV bolus dose or oxytocin 25 IU as an 8 h IV infusion.
The results of analysis of the primary endpoint, the need for additional oxytocic intervention, showed that additional oxytocin intervention was required in 15 (5%) of the subjects receiving carbetocin 100 μg IV compared with 32 (10%) of the subjects in the oxytocin 25 IU group (p=0.031).
The efficacy of carbetocin in the prevention of postpartum haemorrhage following vaginal delivery was established in one randomised, active controlled, double-blind trial. In total 29645 subjects were randomised to receive a single intramuscular dose of either carbetocin 100 μg or oxytocin 10 IU. For the primary endpoint of blood loss of ≥500 mL or use of additional uterotonics, similar rates were obtained in both treatment groups (carbetocin: 2135 subjects, 14.47%; oxytocin: 2122 subjects, 14.38%; relative risk [RR] 1.01; 95% CI: 0.95 to 1.06), demonstrating non-inferiority of carbetocin compared with oxytocin with regard to the primary endpoint.
Paediatric population: In the clinical development of carbetocin for prevention of postpartum haemorrhage following vaginal delivery 151 women between 12 and 18 years of age received carbetocin at the recommended dosage of 100 μg and 162 received oxytocin 10 IU. Efficacy and safety was similar for the two treatment arms in these patients.
Pharmacokinetics: The pharmacokinetics of carbetocin have been investigated in healthy female subjects. Carbetocin shows biphasic elimination after intravenous administration with linear pharmacokinetics in the dose range of 400 to 800 micrograms. The terminal elimination half-life is 33 minutes after intravenous administration and 55 minutes after intramuscular administration. After intramuscular administration, peak concentrations are reached after 30 minutes and the bioavailability is 77%. The mean volume of distribution at pseudo-equilibrium (Vz) is 22 L. Renal clearance of the unchanged form is low, with <1% of the injected dose excreted unchanged by the kidney.
After intramuscular administration of 70 μg carbetocin in 5 healthy nursing mothers, carbetocin concentrations were detectable in milk samples. Mean peak concentrations in milk were below 20 pg/mL, which was approximately 56 times lower than in plasma at 120 min.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicology, genotoxicity and local tolerance. A reproductive toxicity study in rats with daily drug administration from parturition to day 21 of lactation, showed a reduction in offspring body weight gain. No other toxic effects were observed. The indication did not warrant studies on fertility, embryotoxicity or carcinogenicity.
DURATOCIN RTS is indicated for the prevention of postpartum haemorrhage due to uterine atony.
Posology: Caesarean section under epidural or spinal anaesthesia: Withdraw 1 ml of DURATOCIN RTS containing 100 micrograms carbetocin and administer only by intravenous injection, under adequate medical supervision in a hospital.
Vaginal delivery: Withdraw 1 ml of DURATOCIN RTS containing 100 micrograms carbetocin and administer by intravenous injection or intramuscular injection, under adequate medical supervision in a hospital.
Method of administration: For intravenous or intramuscular administration.
Carbetocin must only be administered after delivery of the infant, and as soon as possible after delivery, preferably before the delivery of the placenta.
For intravenous administration carbetocin must be administered slowly, over 1 minute.
DURATOCIN RTS is intended for single use only. No further doses of carbetocin should be administered.
Paediatric population: There is no relevant use of carbetocin in children below 12 years of age. The safety and efficacy of carbetocin in adolescents has not yet been established.
Currently available data are described in Pharmacology: Pharmacodynamics under Actions but no recommendation on a posology can be made.
Overdosage of carbetocin may produce uterine hyperactivity. At single doses up to 800 micrograms tachycardia was observed.
Overdosage of oxytocin may lead to hyponatraemia and water intoxication in severe cases, especially when associated with excessive concomitant fluid intake. As carbetocin is an analogue of oxytocin, the possibility of a similar event cannot be excluded.
Signs of overdose may be the symptoms arising from water intoxication and uterine hyperactivity. Treatment of overdosage of carbetocin consists of symptomatic and supportive therapy.
Pregnancy and labour before delivery of the infant.
Induction of labour.
Serious cardiovascular disorders.
Hypersensitivity to carbetocin or oxytocin or to any of the excipients listed in Description.
Carbetocin is intended for use only at well-equipped specialist obstetrics units with experienced and qualified staff available at all times.
The use of carbetocin at any stage before delivery of the infant is not appropriate because its uterotonic activity persists for several hours. This is in marked contrast to the rapid reduction of effect observed after discontinuation of an oxytocin infusion.
Carbetocin is intended for single administration only, intramuscular or intravenous. In case of intravenous administration, it must be administered slowly over 1 minute. In case of persisting uterine hypotonia or atonia and the consequent excessive bleeding, additional therapy with another uterotonic should be considered. There are no data on additional doses of carbetocin or on the use of carbetocin following persisting uterine atony after oxytocin.
In general, carbetocin should be used cautiously in the presence of epilepsy, migraine, asthma and cardiovascular disease or any state in which a rapid addition to extracellular water may produce hazard for an already overburdened system. The decision of administering carbetocin can be made by the physician after carefully weighing the potential benefit carbetocin may provide in these particular cases. No data is available on the use of carbetocin in patients with eclampsia. Patients with eclampsia and pre-eclampsia should be carefully monitored.
Animal studies have shown carbetocin to possess some antidiuretic activity (vasopressin activity: <0.025 IU/vial) and therefore the possibility of hyponatraemia cannot be excluded, particularly in patients also receiving large volumes of intravenous fluids. The early signs of drowsiness, listlessness and headache should be recognised to prevent convulsions and coma.
Specific studies have not been undertaken in gestational diabetes mellitus.
Effects on ability to drive and use machines: Not relevant.
Pregnancy: Carbetocin is contraindicated during pregnancy and must not be used for the induction of labour (see Contraindications).
Breastfeeding: No significant effects on milk let-down have been reported during clinical trials. Small amounts of carbetocin have been shown to pass from plasma into breast milk of nursing women (see Pharmacology: Pharmacokinetics under Actions). The small amounts transferred into colostrum or breast milk after a single injection of carbetocin, and subsequently ingested by the infant are assumed to be degraded by enzymes in the gut.
Breast-feeding does not need to be restricted after the use of carbetocin.
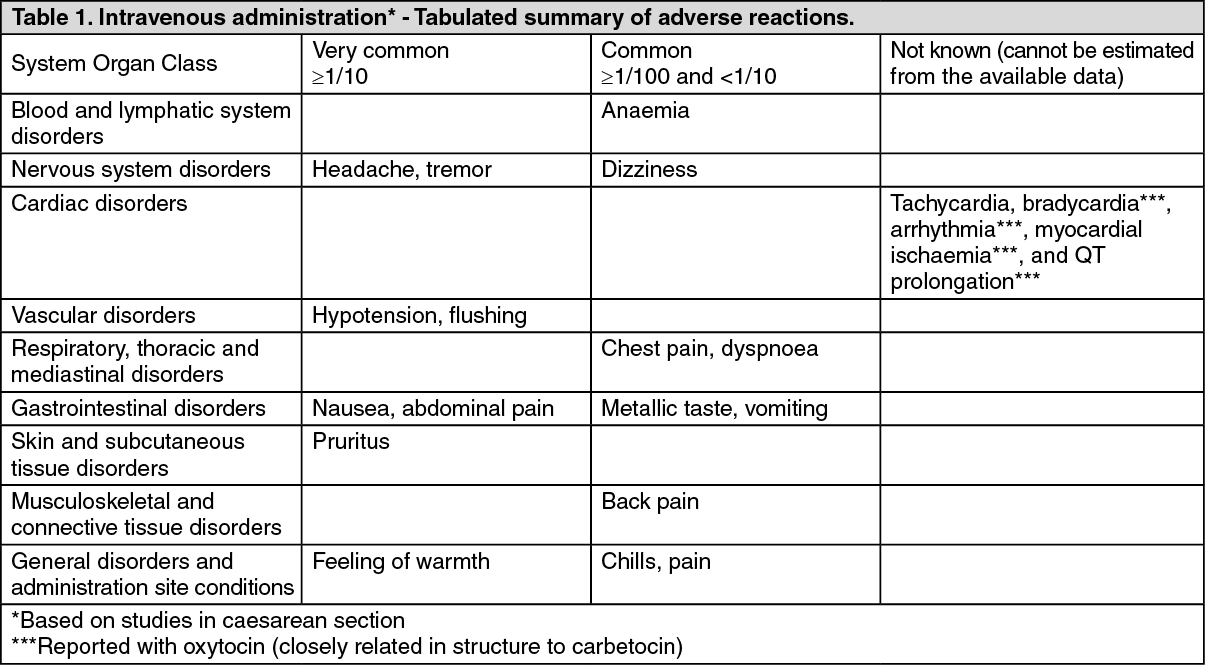
The adverse events observed with carbetocin during the clinical trials were of the same type and frequency as the adverse events observed with oxytocin. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the clinical trials sweating was reported as sporadic cases. (See Table 2.)
Click on icon to see table/diagram/image
During clinical trials, carbetocin has been administered in association with a number of analgesics, spasmolytics and agents used for epidural or spinal anaesthesia, and no drug interactions have been identified. Specific interaction studies have not been undertaken.
Since carbetocin is closely related in structure to oxytocin, the occurrence of interactions known to be associated with oxytocin cannot be excluded: Severe hypertension has been reported when oxytocin was given 3 to 4 hours following prophylactic administration of a vasoconstrictor in conjunction with caudal-block anaesthesia.
During combination with ergot-alkaloids, such as methylergometrine, oxytocin and carbetocin may enhance the blood pressure enhancing effect of these agents. If oxytocin or methylergometrine are administered after carbetocin there may be a risk of cumulative exposure.
Some inhalation-anesthetics, such as halothane and cyclopropane may enhance the hypotensive effect and weaken the effect of carbetocin on the uterus. Arrhythmias have been reported for oxytocin during concomitant use.
Incompatibilities: In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Special precautions for disposal and other handling: DURATOCIN RTS is for intravenous and intramuscular use only.
Only clear solutions practically free from particles should be used.
Any unused product or waste material should be disposed of in accordance with local requirements.
Keep vials in the outer carton, in order to protect from light. Store below 30°C. Do not freeze.
Shelf life: 3 years.
Shelf life after first opening the vial: the solution should be used immediately.
From a microbiological point of view, unless the method of opening/reconstitution/dilution precludes the risk of microbial contamination, the product should be used immediately.
If not used immediately, in-use storage times and conditions are the responsibility of the user.
H01BB03 - carbetocin ; Belongs to the class of oxytocin and analogues. Used in posterior pituitary lobe hormone preparations.
Duratocin RTS soln for inj 100 mcg/mL
5's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
